A verruca that won’t budge is one of the most frustrating foot problems you can have. You try over-the-counter treatments for weeks, nothing happens, and the thing just sits there — sometimes growing, sometimes spreading, always uncomfortable when you walk.
The good news is that verrucae are well understood and there are several effective treatments, including professional options that work when home remedies fail. This guide explains what verrucae are, why they’re so stubborn, and what your options are.
What is a verruca?
A verruca — also called a plantar wart — is a small, rough growth on the sole of the foot caused by the Human Papillomavirus (HPV). Unlike warts on other parts of the body, verrucae grow inward rather than outward because of the pressure placed on the sole of the foot when you stand and walk. This is why they can be painful and why they’re often harder to treat.
Verrucae typically appear as:
- A small, rough, flattened area of skin on the sole of the foot
- Cauliflower-like in texture, sometimes with tiny black dots in the centre (these are small blood vessels, not “roots”)
- Pain when you press on the sides of the growth rather than directly on it — this helps distinguish a verruca from a corn
- Occasionally in clusters, known as mosaic warts
They most commonly appear on the heel, the ball of the foot, or the base of the toes — areas that bear the most pressure.
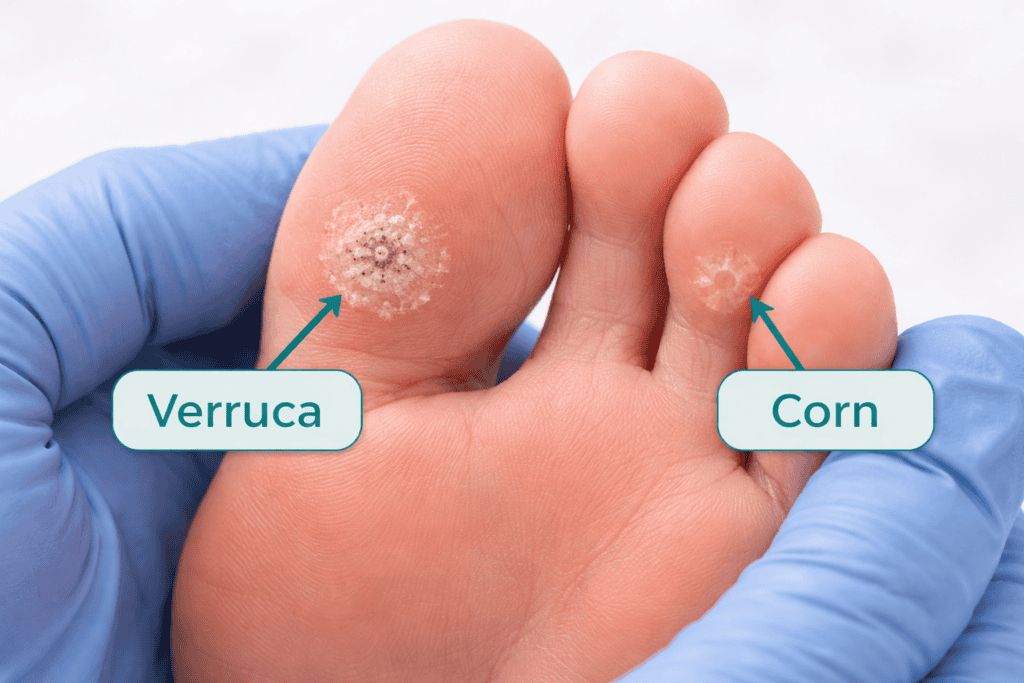
Verruca or corn — how to tell the difference
Verrucae and corns are frequently confused because they look similar and both appear on pressure points. The key differences are:
- Pain on squeezing — press the sides of the growth. A verruca is painful when squeezed from the sides. A corn hurts when pressed directly from above.
- Skin lines — look closely at the skin around the growth. The natural lines of your skin (like fingerprints) continue through a corn but are interrupted by a verruca.
- Black dots — the tiny dark specks sometimes visible in verrucae are capillary blood vessels. Corns don’t have these.
- Surface texture — verrucae have a rough, cauliflower-like surface. Corns are usually smoother with a hard central core.
If you’re not sure what you’re dealing with, a podiatrist can diagnose it in seconds.
How do verrucae spread?
HPV is spread through direct contact with the virus — usually from contaminated surfaces. The virus thrives in warm, moist environments, which is why verrucae are particularly associated with:
- Swimming pools and changing rooms
- Communal showers
- Gyms and sports facilities
The virus enters the skin through tiny cuts or abrasions. People with weakened immune systems, children and teenagers are more susceptible — though anyone can develop a verruca.
Verrucae can also spread to other parts of your own foot, particularly if you scratch them or pick at them. They are contagious to others, though the risk is relatively low in normal social contact.
Will a verruca go away on its own?
Yes — many verrucae do resolve on their own as the immune system eventually recognises and eliminates the virus. In children, this often happens within a year or two. In adults, it can take considerably longer — sometimes several years — and some verrucae never resolve without treatment.
The problem is that while you’re waiting, the verruca may grow larger, become more painful, or spread. Most people prefer to treat rather than wait.
Over-the-counter verruca treatments
For small, single verrucae that aren’t causing significant pain, over-the-counter treatments are a reasonable first step.
Salicylic acid
This is the most common and best-evidenced home treatment. Available as gels, paints, plasters and creams (brands include Bazuka, Wartner and own-brand products), salicylic acid works by gradually breaking down the hardened skin of the verruca.
For best results:
- Soak the foot in warm water for 5 minutes to soften the skin
- File the surface of the verruca with an emery board or pumice stone to remove dead skin
- Apply the salicylic acid treatment to the verruca only, avoiding surrounding healthy skin
- Cover with a plaster or dressing
- Repeat daily — consistency is essential
Treatment can take 8 to 12 weeks or longer to work. Many people stop too early. If there’s no improvement after 12 weeks, it’s time to try something else.
Cryotherapy (freeze sprays)
Over-the-counter freeze sprays such as Wartner or Scholl Freeze work by freezing the verruca tissue. They are less cold than the liquid nitrogen used by podiatrists, so they are generally less effective for stubborn or deep verrucae — but they can work for smaller ones.
Follow the instructions carefully and don’t reapply more frequently than recommended, as this can damage surrounding healthy skin.
Professional verruca treatments
If home treatment hasn’t worked after 2 to 3 months, or if your verruca is large, painful or spreading, a podiatrist can offer more effective options.
Professional cryotherapy (liquid nitrogen)
This is one of the most common professional treatments. The podiatrist applies liquid nitrogen to the verruca, which freezes it at a much lower temperature than home freeze sprays. The frozen tissue dies and eventually falls away.
Treatment typically requires multiple sessions — usually every 2 to 3 weeks — and can be uncomfortable, though most people tolerate it well. Success rates are good, though not guaranteed for all verrucae.
Swift microwave therapy
Swift is one of the most exciting recent developments in verruca treatment. A small probe delivers focused microwave energy to the verruca tissue, heating it to a precise temperature that stimulates the immune system to recognise and attack the HPV virus.
Unlike traditional treatments, Swift targets the virus itself rather than simply destroying the skin tissue. Clinical studies show success rates of around 76% after three treatments — significantly better than cryotherapy for many verruca types. Treatment takes seconds per verruca, requires no dressings or recovery time, and most patients need 3 to 4 sessions.
Swift is available at specialist podiatry practices across the UK and is particularly recommended for long-standing or recurrent verrucae.
Needling (falknor’s needling procedure)
This procedure involves puncturing the verruca with a fine needle under local anaesthetic, which breaks up the tissue and exposes the HPV virus to the immune system beneath the skin. This triggers an immune response that can clear the verruca and any others on the foot.
Needling is particularly useful for multiple or mosaic verrucae, as treating one can resolve others simultaneously. It requires only a single treatment in most cases, though results are not instant — it can take several months for the immune response to fully clear the verruca.
Surgical removal
Surgical excision of verrucae is now rarely recommended as a first-line treatment because it carries a risk of scarring and recurrence rates are similar to other treatments. It may be considered for very large or resistant verrucae where other treatments have failed.
When should you see a podiatrist?
You should seek professional advice if:
- Home treatment hasn’t worked after 2 to 3 months
- The verruca is large (larger than 1cm), spreading or multiplying
- The verruca is causing significant pain when walking
- You have diabetes, poor circulation or any condition affecting your immune system — in these cases you should not use over-the-counter treatments and should seek professional advice from the outset
- You are not sure whether it is a verruca
- The verruca is in a location where it bleeds or frequently breaks down
How to reduce the risk of verrucae
- Wear flip-flops or pool shoes in communal changing rooms and pool areas
- Don’t share towels, socks or footwear
- Keep feet clean and dry
- Cover any cuts or abrasions before using communal facilities
- If you have a verruca, cover it with a waterproof plaster when swimming or using communal showers to reduce the risk of spreading it to others
Find a podiatrist near you
If you have a verruca that isn’t responding to home treatment, a podiatrist can assess it and recommend the most appropriate treatment — including Swift microwave therapy where available. Search our directory to find HCPC-registered specialists in your area.
This article is for general information only and does not constitute medical advice. Always consult a qualified, HCPC-registered practitioner for diagnosis and treatment of any foot condition.
Written by
FootcareUK Editorial Team
Our articles are written and reviewed by qualified foot health professionals including podiatrists and chiropodists. The FootcareUK editorial team is committed to providing accurate, up-to-date information to help you make informed decisions about your foot health care.